
Epidemiology
Half of all brain and spinal cord tumors are metastatic
Most frequent primary CNS tumors: Meningiomas
Glioblastoma multiforme
Clinical manifestations
Headache, often worse at night or early morning
Seizures, with tumors involving cerebral cortex
Mental changes (e.g., deficits in memory, concentration, reasoning, etc.)
Focal neurological symptoms, related to involvement of specific brain regions
Symptoms related to increased intracranial pressure
i. Presence of a space-occupying mass within the cranial cavity
ii. Blockage of CSF flow
iii. Edema around the tumor (peri tumoral edema)
Special features of brain tumors
i. Malignant CNS tumors do not metastasize outside the cranial cavity.
ii. Clinical consequences depend on infiltrative behavior and location.
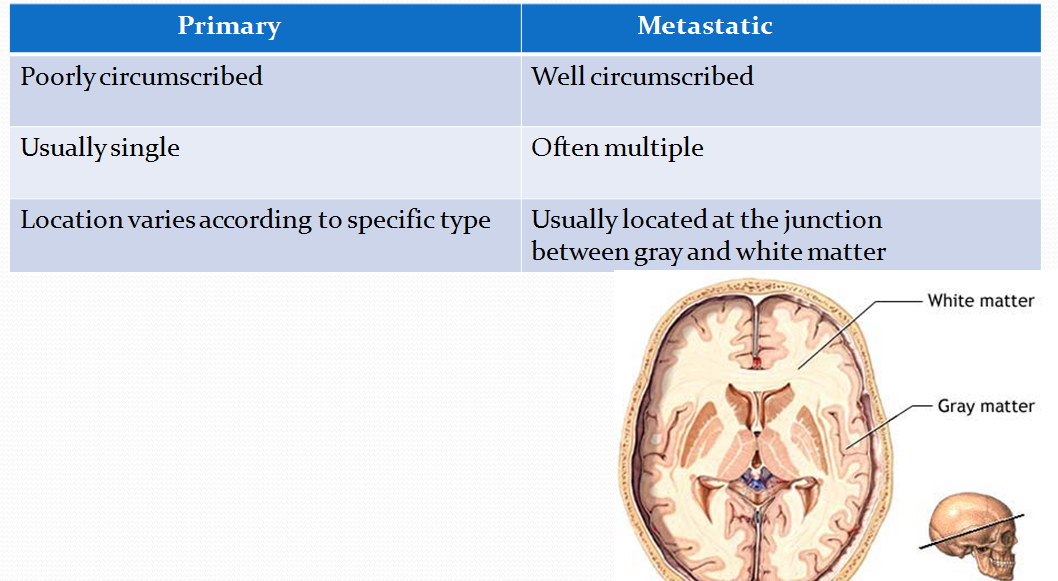
Differences Between Primary and Metastatic Tumors
Astrocytomas
a. Originate from astrocytes and exhibit
i. Fibrillary background
ii. Immunoreactivity for glialfibrillary acidic protein (GFAP)
iii. Diffuse (ill-demarcated) pattern of growth
a. Fibrillary astrocytomas
Grading is important for both prognosis and treatment. Most frequent systems
Four grades based on nuclear atypia (pleomorphism),
-mitoses, necrosis, and vascular endothelial hyperplasia (VEH)
Grade 1-2 astrocytomas are well differentiated astrocytomas
Grade 3 astrocytomas are anaplastic astrocytomas
Grade 4 astrocytomas are called glioblastoma multiforme (GBM)
GBM is the most cormmon CNS primary malignancy
Most common location: white matter
Histology: marked nuclear atypia, mitoses, necrosis, and VEH
Characteristic histo pathological feature: pseudopalisading necrosis
VEH is often florid, giving rise to glomeruloid formations

Glioblastoma multiforme has a tendency to cross the midline
by involving the corpus callosum, hence k/a"Butterfly glioma"

Anaplastic astrocytoma showing marked nuclear pleomorphism

b. Pilocytic astrocytoma
Benign astrocytic tumor of children and young adults
Locations: posterior fossa (cerebellum) and diencephalon
Often presents as a cystic lesion with a mural nodule


Histology:
-spindly neoplastic astrocytes with long bipolar processes
-tumors rich in Rosenthal fibers (thick corkscrew-like eosinophilic structures, which derive from hypertrophic processes of astrocytes)
Favorable prognosis for posterior fossa tumors

Oligodendroglioma
Glioma of oligodendroglial origin
Occurs in 30- to 50-year-old patients
Location: white matter of cerebral hemispheres adjacent to neocortex

Often manifests with seizures
Characteristic histopathology
i. Neoplastic cells are similar to oligodendroglia
ii. Pronounced perinuclear halo: "fried-egg" appearance

iii. Prominent capillary network in a chickenwire pattern
Slow-growing tumors that allow long survival (average 5-10 years)
Recur after surgery and degenerate into high-grade gliomas over time

Ependymoma
Glioma of ependymal origin
Location
1. Children: fourth ventricle
ii. Adults: lateral ventricle or spinal canal
Gross appearance: circumscribed tumors with papillary architecture

Histology: neoplastic cells resemble ependymal cells. Characteristic features:
i. Ependymal rosettes

ii. Perivascular pseudo rosettes

Often presents with obstructive hydrocephalus, when present in the fourth ventricle
Tend to recur after surgery and acquire more aggressive behavior
Meningioma
Originates from meningothelial cells of the arachnoid
Tumors of adulthood (women> men), rare in children
May develop at any meningeal site. Most frequent are dural convexities
Gross: attached to the dura,
pushes underlying brain
without invasion

Microscopic
i.Spindle-shaped cells with indistinct borders (syncytial)
ii. Cells arranged in whorls or fascicles
iii. Psammoma bodies frequent


Generally, good prognosis
Tumors in some location may not be amenable to complete resection
Primitive neuroectodermal tumors (PNET)
Highly undifferentiated; originate from a primordial neuroglial precursor
Variably named, depending on location in the brain
Most frequent PNETs: medulloblastoma and
retinoblastoma
All PNETs share the following features:
i. Develop in children
ii. Histology: blue, small, round cell tumors, with pseudorosettes
iii. Highly aggressive but responsive to radiation therapy
.
Histo:

Medulloblastoma arises in the cerebellar vermis (midline location)
i. Grows rapidly and spreads through CSF
ii. Resection and radiation therapy allow 5-year survival of 75%.

Schwannoma
Originates from Schwann cells of cranial or spinal nerves
Associated with NF type II
Most frequent location: eighth cranial nerve
cerebellopontine angle(CPA)
Manifests characteristically with loss of hearing and tinnitus

Histology
i. Spindle cells arranged in hypercellular Antoni A areas, alternating with hypocellular Antoni B areas
ii. Verocay bodies: parallel rows of neoplastic Schwann cells

Verocay bodies
Neoplastic cells are immunoreactive for a protein called S-100
Good prognosis after surgical resection

Craniopharyngioma
Arises from the remmanants of Rathke’s pouch
Patients affected are usually children or young adults
Location: within the suprasellar/diencephalic region
Gross: craniopharyngiomas are cystic or partially-cystic with solid areas.

Histo: nesting of squamous epithelium bordered by radially arranged cells.
resembles adamantinoma, the most common tumor of the tooth

Benign but tends to recur after resection
T/T:
Trans-sphenoidal resection of the tumor.
Investigations of Brain tumors:
1. CT/MRI Head
allows localization of the tumor.
MRI has value in investigation of posterior fossa tumors and brain stem
2. CXR:
provides evidence of primary lung tumor
T/t
1.Medical: Relief of ICP is reqd. when surgery is not possible or
when life is threatened before diagnosis is revealed.
Dexamethasone is used.
2. Surgical:
Main stay of t/t
3. Radiotherapy and Chemotherapy
No comments:
Post a Comment